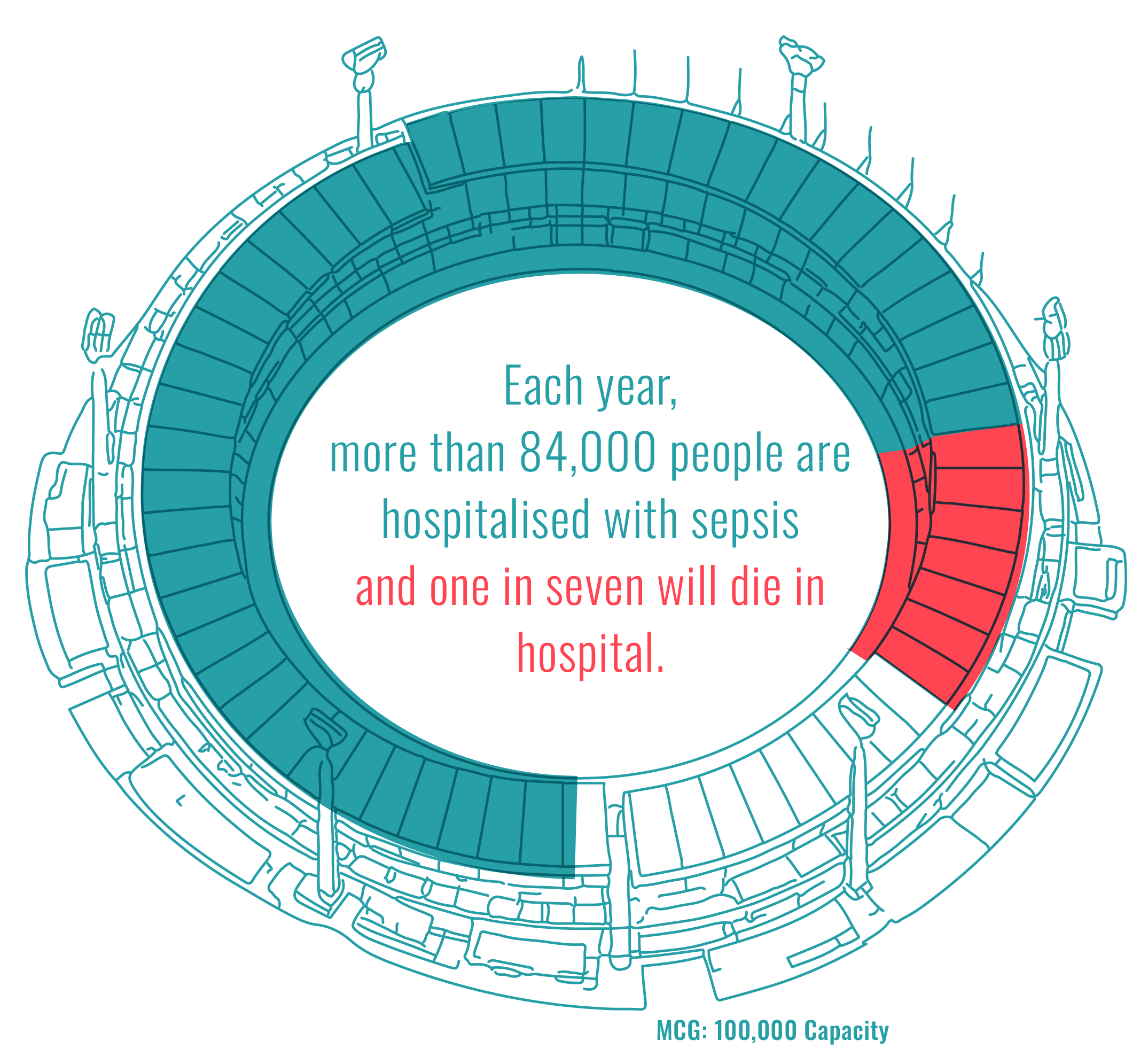
Every 20 minutes an Australian is admitted to intensive care with sepsis. Each year, more than 84,000 people are hospitalised with this life-threatening condition, and one in seven will die in hospital. Sepsis claims more lives than common cancers and causes four times more deaths than road trauma. Despite this burden, significant questions remain about how best to prevent, recognise and treat sepsis, and how to support people after survival.
Top 10 Sepsis Research Priorities
-
Sepsis can impact the brain in multiple ways, causing both acute and long-term neurological complications that increase morbidity and mortality and can impair cognitive function. Cognitive impairment is common, yet the underlying mechanisms remain poorly understood.
-
Description text goes here
-
Description text goes here
-
Item description
-
Item description
-
Item description
-
Item description
-
Item description
-
Item description
-
Item description
Shaping Sepsis Care
The National Critical Care Research (NCCR) Collaboration is committed to building a Learning Healthcare System that enhances outcomes for patients and families while strengthening the effectiveness and efficiency of clinical care. Central to this commitment is ensuring the research is guided by the priorities of those most affected: people with lived experience of sepsis, their carers, and the healthcare professionals who care for them.
To achieve this, NCCR has led Shaping Sepsis Care, a Priority Setting Partnership (PSP) for sepsis research in Australia, delivered in collaboration with the UK-based James Lind Alliance (JLA). This partnership brought together consumers and healthcare professionals to jointly identify and prioritise the unanswered questions that matter most in sepsis care. Incorporating lived experience alongside clinical expertise helps ensure that research priorities are relevant, balanced and grounded in real-world needs.
This structured process resulted in the identification of the Top 10 national sepsis research priorities, as agreed by patients, carers, and healthcare professionals.
The findings in this report will inform the development of the Australian Sepsis Research Roadmap, providing clear direction for researchers, funders and policymakers. It is our hope that by aligning future research investment with shared national priorities, Shaping Sepsis Care can accelerate evidence generation, strengthen funding advocacy, and ultimately improve care and outcomes for all Australians affected by sepsis.
We extend our thanks to our funders, partners and all those who contributed to Shaping Sepsis Care and affirm our commitment to stewarding these shared priorities transparently, responsibly and in the interests of better outcomes for people affected by sepsis.

A/Prof Kimberley Haines
Shaping Sepsis Care Lead - Western Health/ University of Melbourne

Prof Andrew Udy
NCCR Chair- Alfred Health/ Monash University
Shaping Sepsis Care: Purpose and Approach
Shaping Sepsis Care is a national Australian initiative designed to identify and prioritise the most important unanswered research questions in sepsis care. The initiative brings together people with lived experience of sepsis, carers and healthcare professionals to ensure that future research is informed by a broad range of perspectives and grounded real-world need.
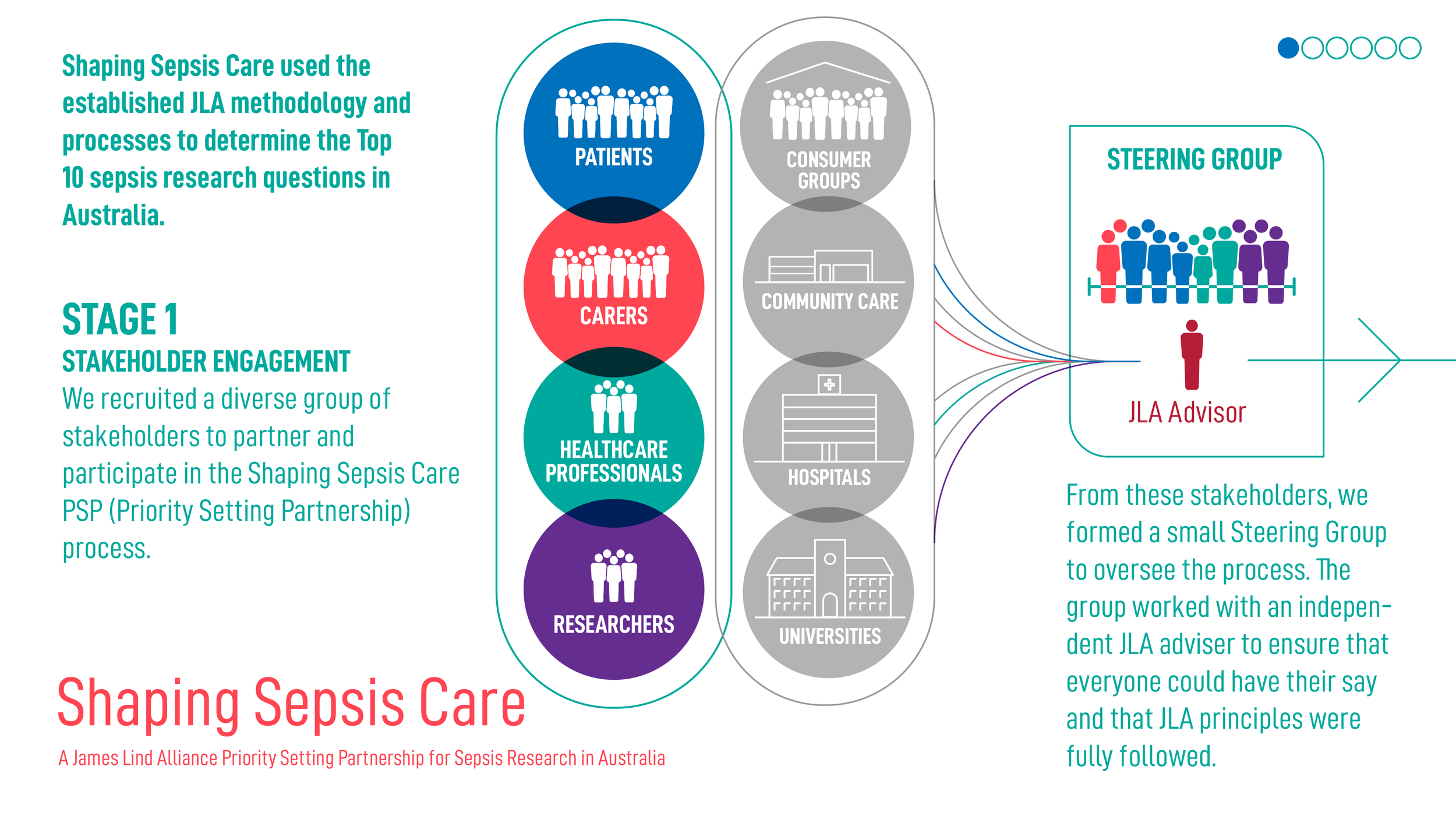
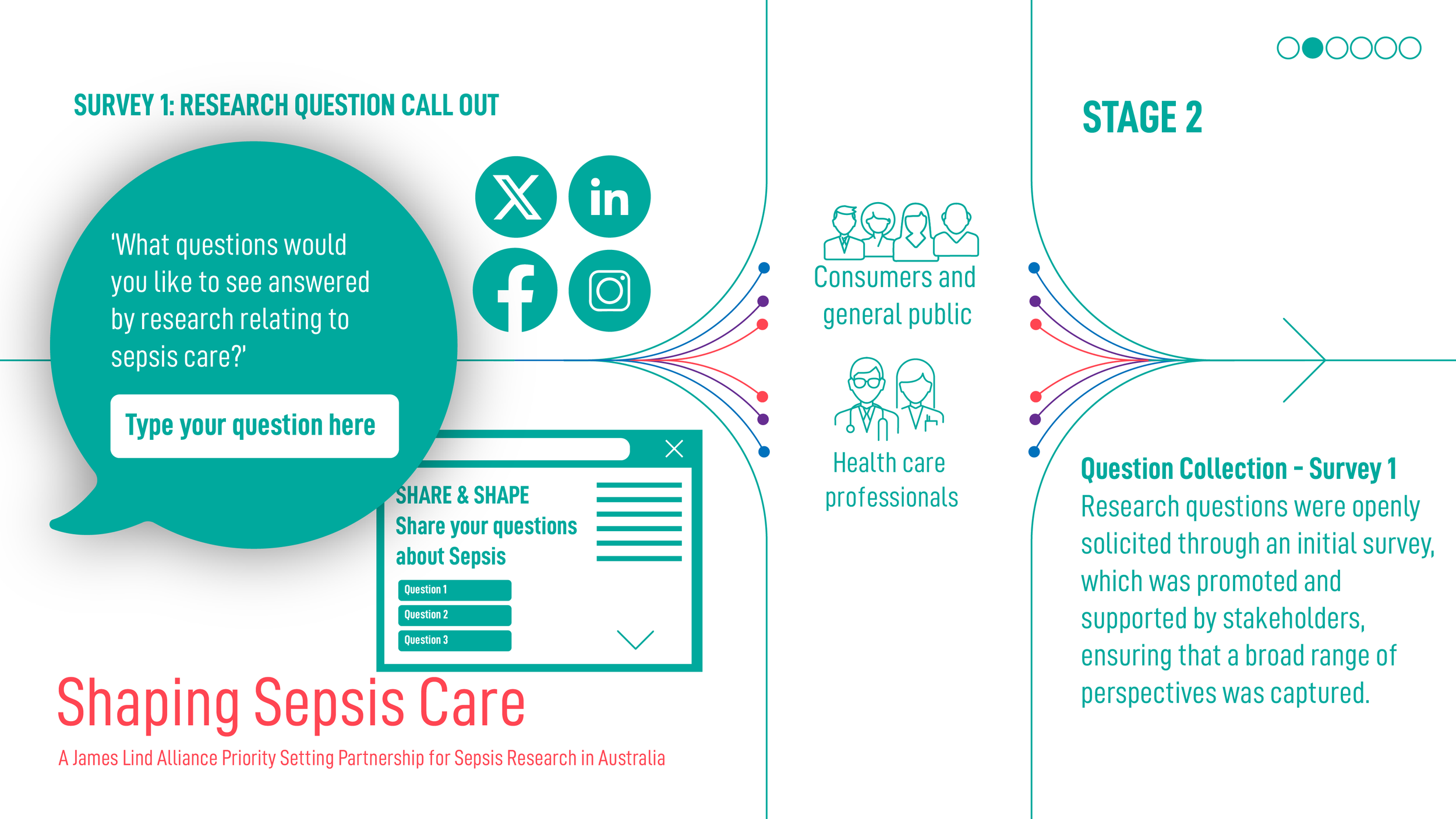
Delivered as a Priority Setting Partnership (PSP) in collaboration with the James Lind Alliance (JLA), Shaping Sepsis Care applies an established and internationally recognised methodology to gather, refine and prioritise research questions. This structured process resulted in the identification of the Top 10 national sepsis research priorities, as agreed by patients, carers, and healthcare professionals.
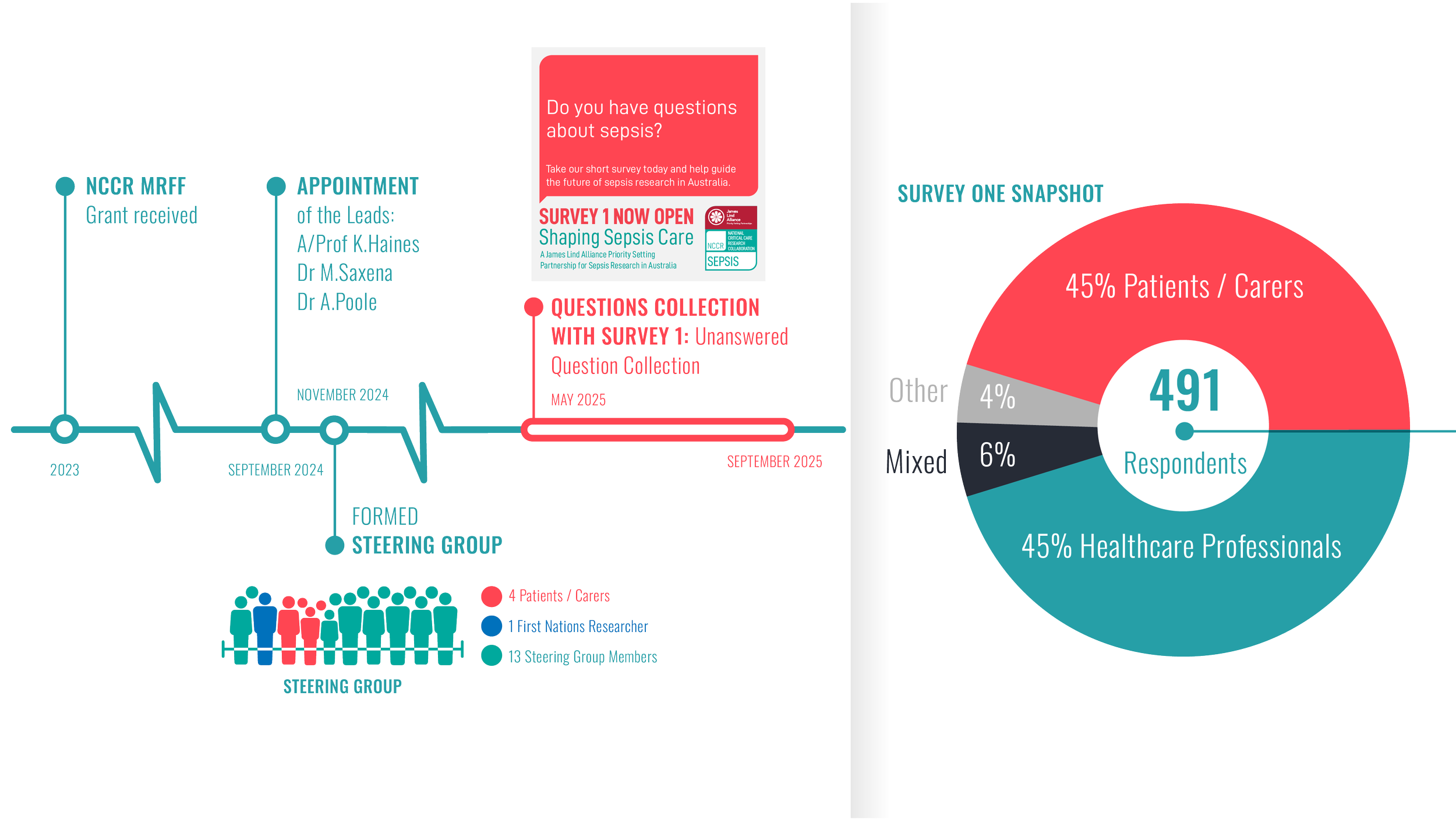
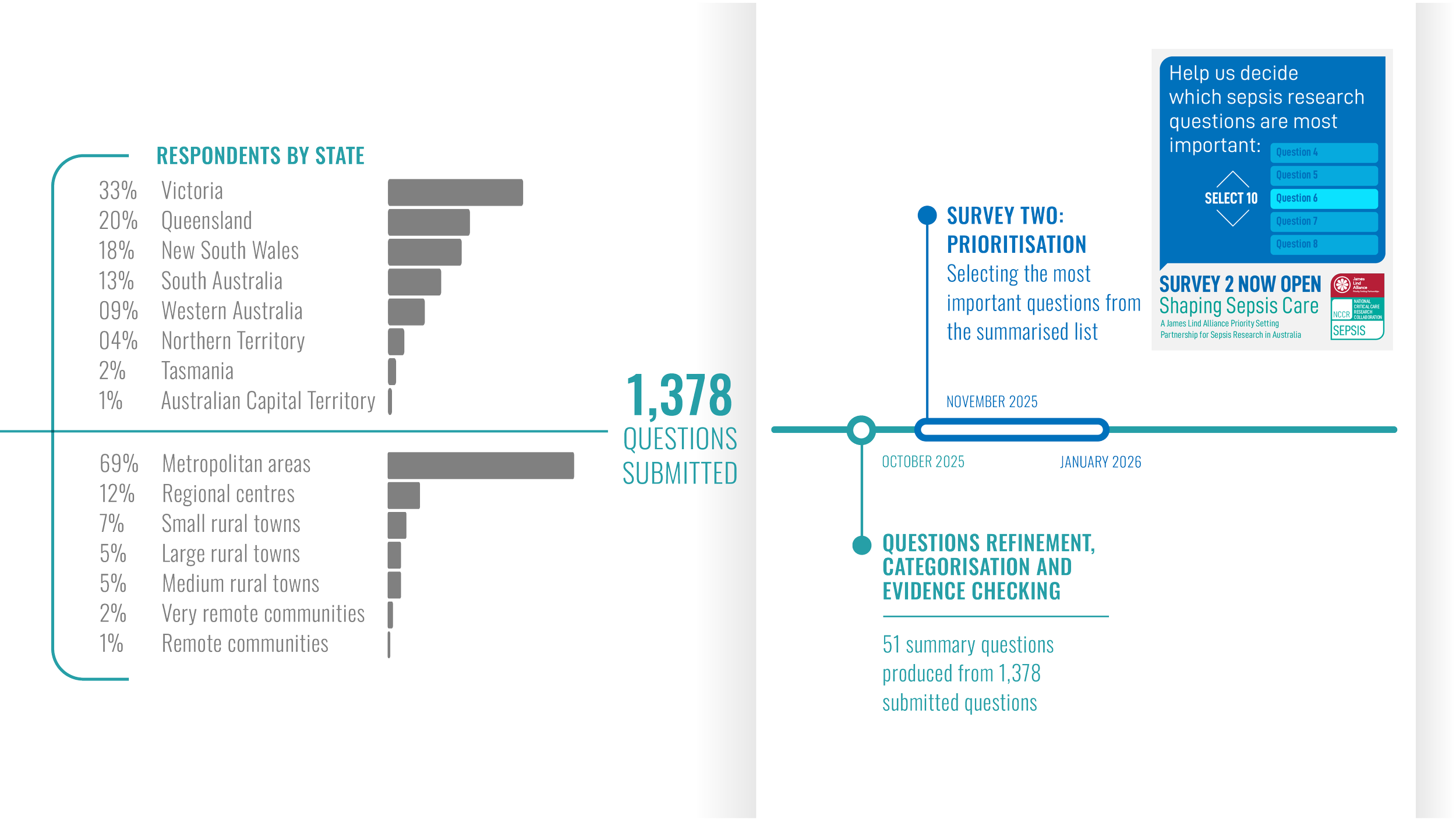
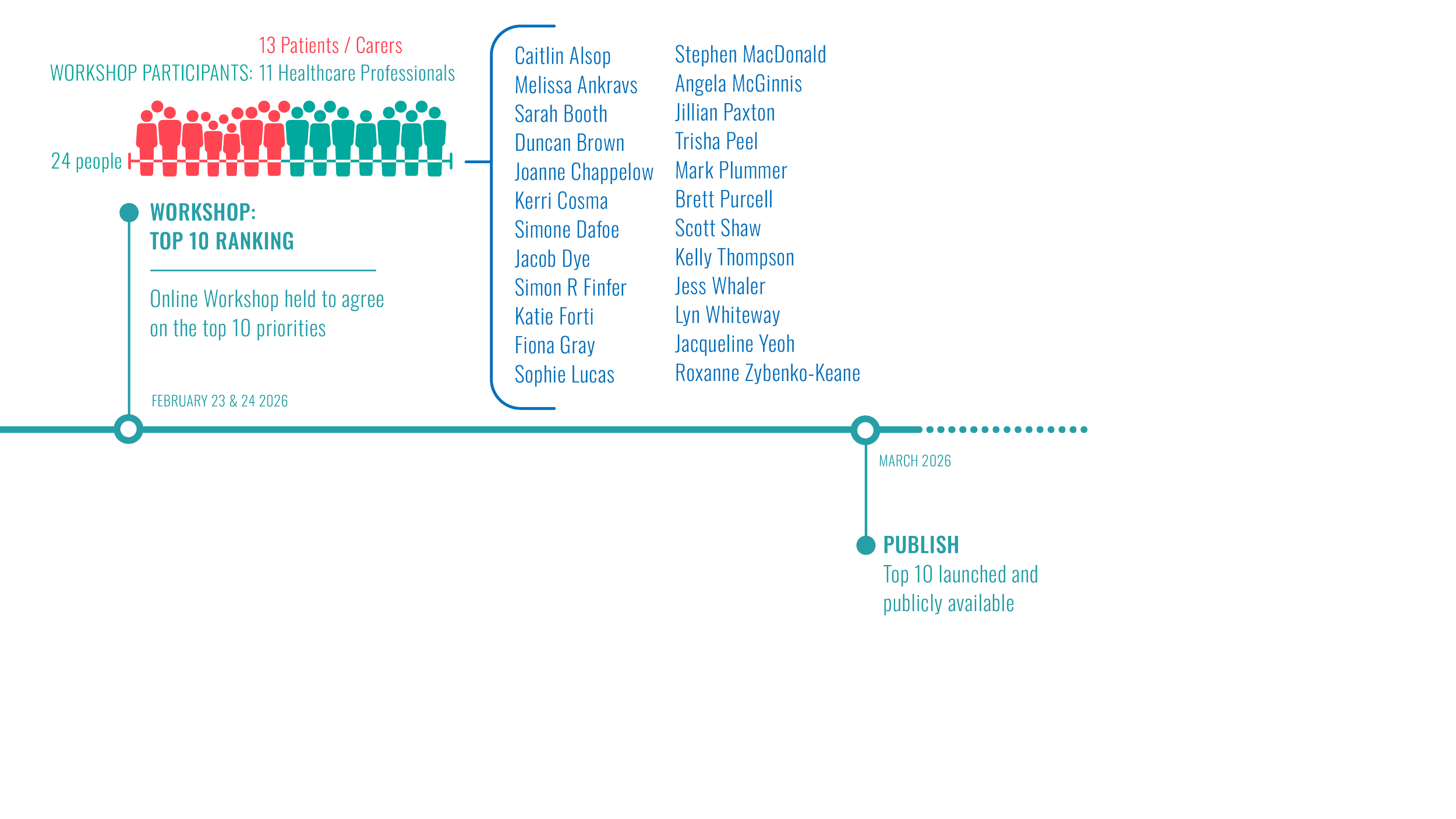
Shaping Sepsis Care: Project Timeline

Additional Research Priorities
Continued by ranking
-
Description text goes here
-
Description text goes here
-
Description text goes here
-
Item description
-
Item description
-
Item description
-
Item description
-
Item description
-
Item description
-
Item description
Summary of TOP 50 questions by category
-
What happens during sepsis to sometimes cause post-sepsis syndrome?
How does sepsis affect the brain?
How and why do some people with sepsis become seriously ill very quickly?
How and why do some infections lead to sepsis?
-
Which health problems might increase the risk of developing sepsis (e.g. infections, poor immunity, surgery and other health conditions)?
Which infections are most likely to lead to sepsis?
Are some people at greater risk of developing sepsis because of their genetic make-up?
Are there factors which protect people from developing sepsis?
What factors (e.g. genetics, age or ethnic background) influence whether a person recovers or dies from sepsis, and how well a person recovers?
Are there particular groups of people who are more at risk of developing sepsis (e.g. because of their age, gender, lifestyle, or ethnic background)?
How can the negative impacts of social disadvantage on the risk of developing sepsis and treatment outcomes be reduced?
What are the best ways to predict which patients are at greatest risk of developing sepsis, and who is likely to recover, or become seriously ill or die?
-
How often is sepsis recognised? Why does it get missed? What would help improve the recognition of sepsis?
How can the speed, accuracy and consistency of diagnosing sepsis be improved?
Is there a tool or test to identify people who are likely to develop post-sepsis syndrome? Would this help to identify who will need follow-up care?
Is there a way to diagnose sepsis earlier before it becomes serious?
Can diagnostic tests be developed for sepsis that can be used wherever the person is receiving care (e.g. in a GP surgery, hospital, ambulance or at home)?
-
What are the costs to society of sepsis, including healthcare costs and lost productivity?
-
What is the role of family members and carers in identifying sepsis in their loved one?
How can family members/ carers and hospital staff work together to provide care for the person with sepsis?
-
What are the best ways for the health system to monitor people after sepsis and provide follow-up care?
How can access to healthcare, diagnosis and treatment be improved for First Nation people with sepsis?
How can discharge from hospital after sepsis be improved so people have the information and support they need?
Are outcomes worse for people with sepsis living in rural and remote areas? How can their diagnosis, treatment and care be improved?
How can communication and care co-ordination be improved across the teams of health professionals caring for people with sepsis?
Why is post-sepsis syndrome not always recognised or accepted within the health system?
Would treatment before admission to hospital (e.g. provided by GPs or paramedics), improve outcomes for people with sepsis?
What are the barriers to people with sepsis receiving rapid treatment once diagnosed, and how can these be overcome?
-
What lifestyle changes can people make (e.g. diet and exercise) to manage post-sepsis syndrome?
-
Does sepsis affect the immune system, increasing the risk of infections?
Does sepsis during pregnancy affect the birth and/ or postnatal recovery?
How can the risk of developing long-term health conditions after sepsis be reduced? How are these conditions best managed following sepsis?
What are the best ways to educate the community to raise awareness of sepsis?
What are the best ways to measure the outcomes of treatment for sepsis in research?
How likely are people to get sepsis again?
What does recovery from sepsis typically look like and how long does it take? How often do people make a full recovery?
-
Would treating sepsis in the early stages improve outcomes and can this prevent people from becoming seriously ill?
Are there ways to prevent people at high risk from getting sepsis again?
Are there ways to prevent people from developing sepsis?
What are the best ways to help people with sepsis to recover (e.g. with support from physiotherapists, dieticians)?
Do complementary therapies (e.g. acupuncture) benefit people with sepsis?
What are the best approaches to treating people with sepsis in intensive care to support organ function?
How can the source of infection be identified rapidly? Does this testing and targeted treatment improve outcomes for people with sepsis?
Are there ways to prevent post-sepsis syndrome by treating the person while they have sepsis?
What range of symptoms do people experience following sepsis, including as part of post-sepsis syndrome? How is this best diagnosed, treated and managed?
Are there ways to tailor treatment of sepsis to the individual (e.g. based on blood markers or other observable characteristics)?
What are the safest and most effective ways to treat sepsis using antibiotics?
-
What are the psychological impacts of caring for someone with sepsis? What forms of psychological support would benefit family members and carers?
What forms of social care and support would benefit people who have recovered from sepsis and their families?
What are the psychological impacts of having sepsis? What are the best ways to treat and manage people's anxiety, depression and/or PTSD (post-traumatic stress disorder)?
What are the long-term impacts of sepsis on people's quality of life, including financial and social impacts? How can people's quality of life be improved?
Leadership, Governance and Oversight
Shaping Sepsis Care is an initiative of the National Critical Care Research (NCCR) Collaboration, a Medical Research Future Fund (MRFF) supported project focused on strengthening outcomes, efficiency and translation in critical care.
The project was jointly led by Clinical Leads A/Prof Kimberley Haines, Dr Manoj Saxena and Dr Alex Poole, working closely with the JLA Adviser and the project coordinators. Together, they guided delivery of the partnership, ensured adherence to JLA methodology, and supported the dissemination of the findings to the researchers, funders and policymakers.
The JLA Adviser for Shaping Sepsis Care was Dr Jonathan Gower, who acted as an independent and neutral facilitator. This role ensured that the process was conducted in a fair and transparent manner, with balanced input from patients, carers and healthcare professionals.
Strategic oversight was provided by a multidisciplinary Steering Group comprising sepsis survivors, carers, healthcare professionals and researchers. Members contributed lived experience, clinical and research expertise, and link to professional and community networks. The Steering Group included an Aboriginal researcher whose participation supported an environment of shared respect, understanding and knowledge, alongside members drawn from a range of professional organisations and care settings.
NCCR is committed to engaging with and learning alongside First Nations peoples as partners in this work, and to conducting the project in a manner that supports respectful collaboration and knowledge sharing.
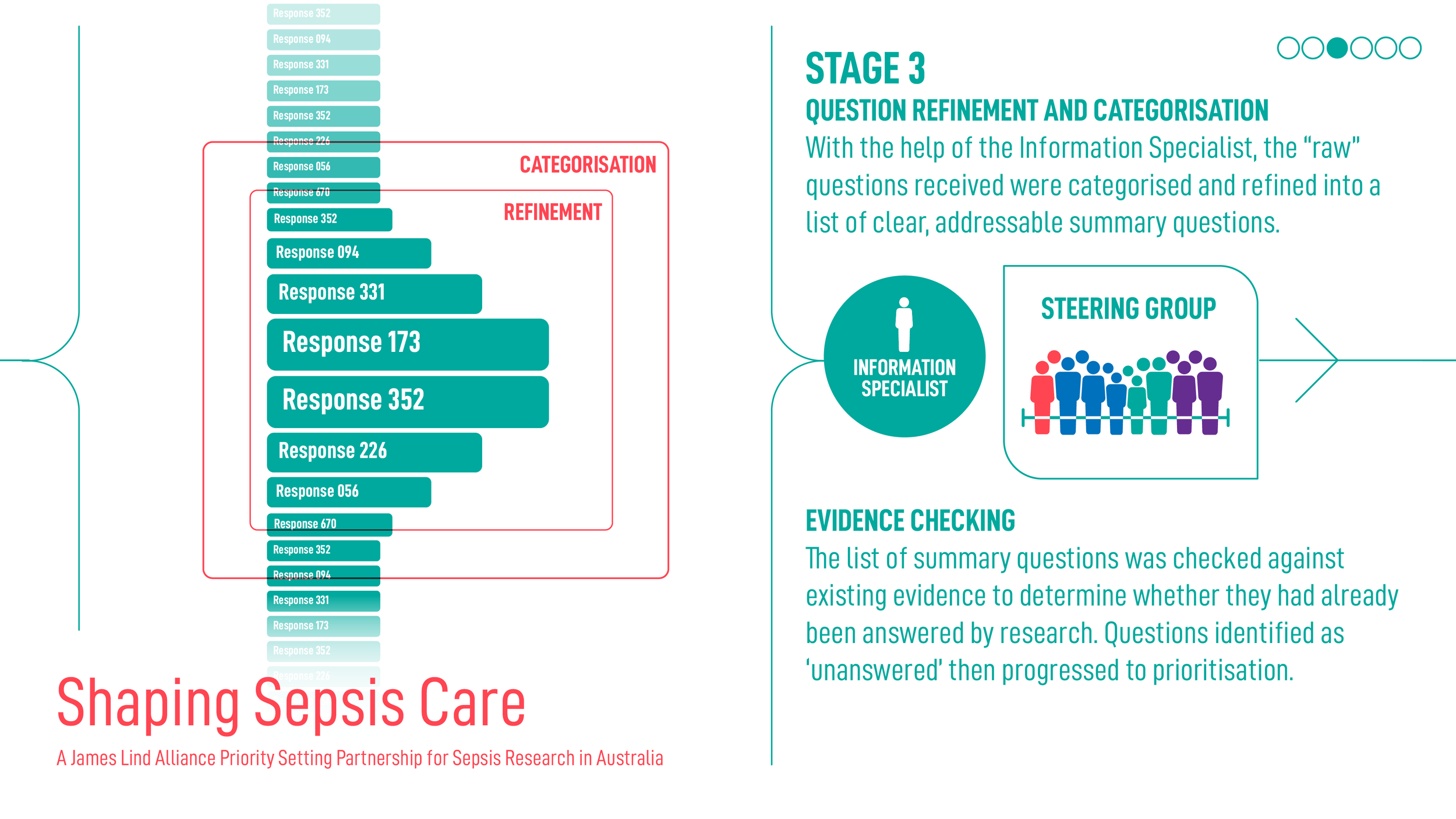
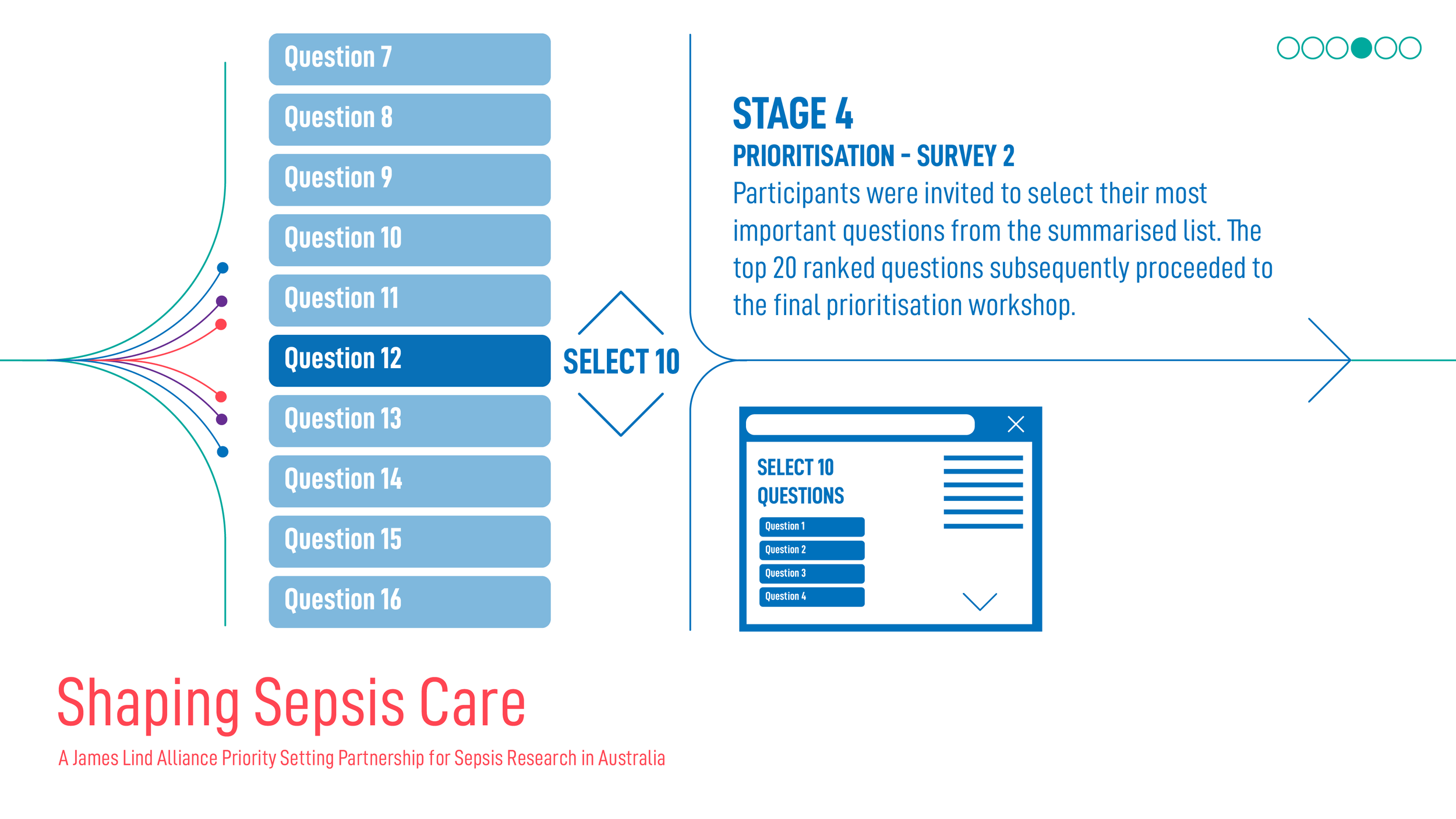
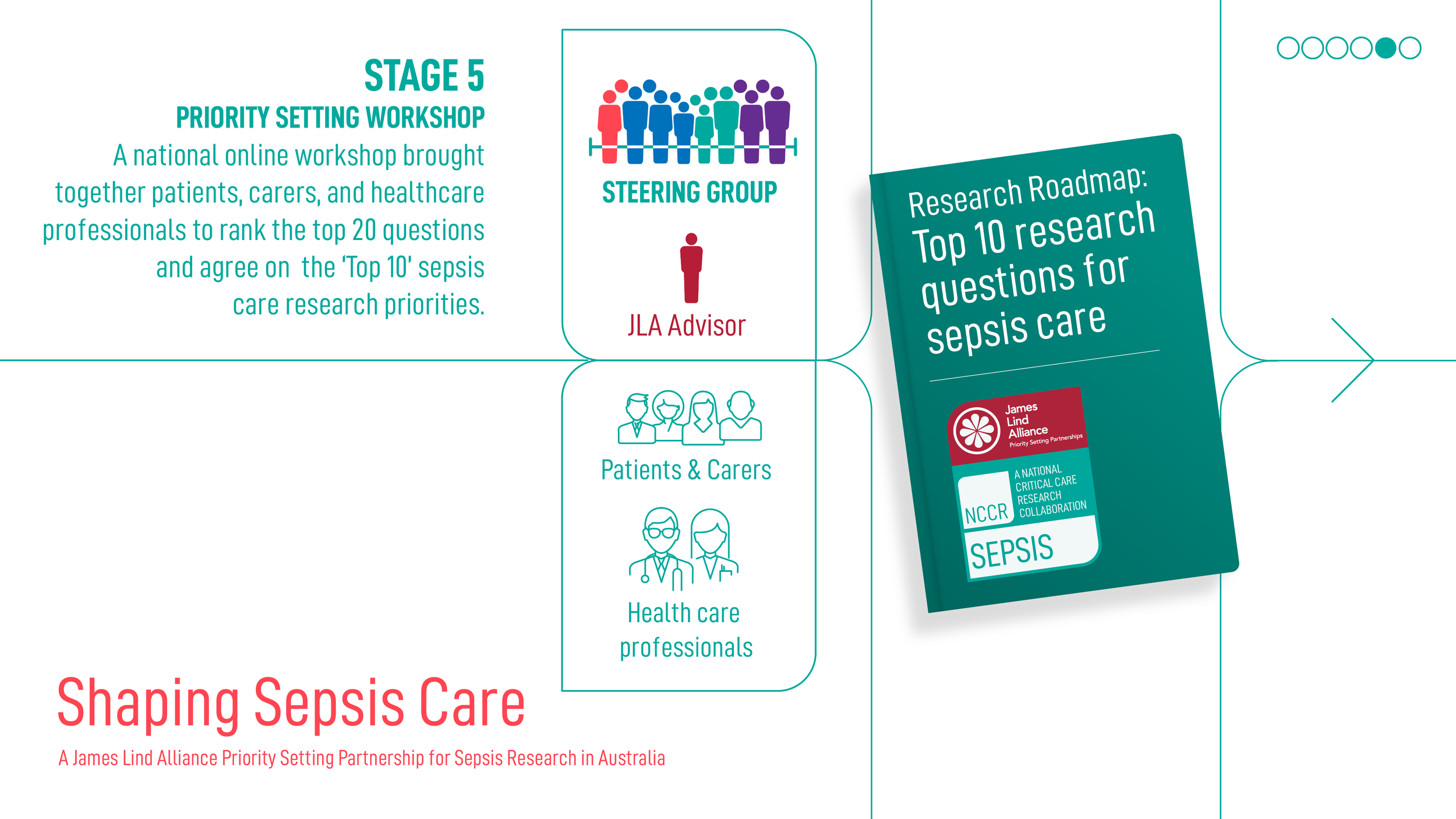
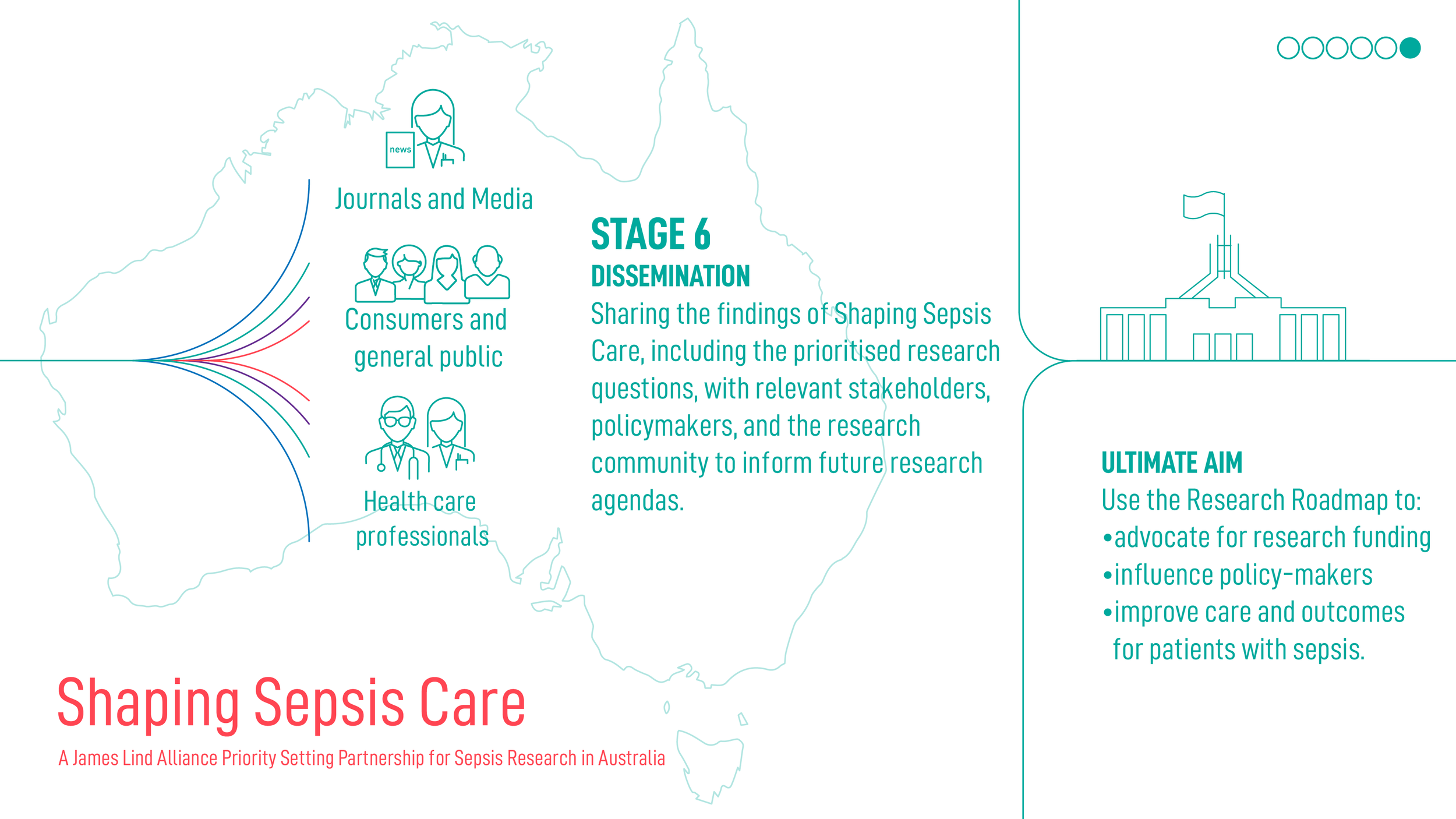
Shaping Sepsis Care: JLA Project Process
Acknowledgements
Shaping Sepsis Care is the result of a national collaboration.
We acknowledge the leadership of our James Lind Alliance Advisor, clinical leads and Steering Group, whose dedication shaped a rigorous and inclusive priority-setting process.
We thank the many organisations and individuals who shared and completed the surveys across Australia. Together, your contributions have shaped the Top 10 priorities and anchored them in lived experience and clinical insight.

This artwork was created by Anmatjere artist Curtis Haines for NCCR. It symbolises a place to come together and talk about sepsis: the green section represents people coming from outside Central Australia, while the brown section represents bush mob. Both groups are journeying toward a central meeting point to collaborate.
Partners